Chronic headache or migraine that won't quit? It may be coming from your neck. Discover cervicogenic headache treatment in Muscat at CBP Precision Spine.
Dr. Coralie Goubier
The Headache Most Doctors Miss
You've tried everything. Paracetamol. Stronger painkillers from the pharmacy. Maybe a neurologist appointment that ended with "tension headache" or "migraine" and a prescription that helps for a few hours. You've cut out caffeine. You've tracked food triggers. You've slept more, slept less, drunk more water, sat in dark rooms.
And the headaches keep coming. Two, three, sometimes five days a week. They start at the base of your skull, climb up the back of your head, and settle behind one eye. They get worse when you sit at your desk for too long. They get worse when you look down at your phone. They get worse when you turn your head a certain way.
If this sounds familiar, there is a very high probability that what you have isn't a migraine at all. It's a cervicogenic headache — a headache that originates in the neck, not the brain. And it accounts for an estimated 15 to 20 percent of all chronic headaches, with office workers disproportionately affected.
In the Middle East specifically, recent research found that 35.5% of patients presenting with headaches actually have a secondary headache — meaning a headache caused by something else in the body, with cervicogenic headaches being one of the most common subtypes. That's roughly one in three. Yet most patients in Muscat will go years before anyone examines their neck as the source.
This article explains why that happens, how to tell the difference between a true migraine and a headache from your neck, and what actually works to fix it.
What a Cervicogenic Headache Actually Is
The medical definition is precise. A cervicogenic headache is a headache caused by a disorder of the cervical spine — the seven vertebrae in your neck — or the soft tissues around it. The pain starts in the neck or the base of the skull and refers up into the head, often presenting in ways that look almost identical to a migraine or tension headache.
The mechanism is well understood. The nerves from the upper cervical spine (specifically C1 to C3) share a pathway with the trigeminal nerve in something called the trigeminal-cervical nucleus. When the upper neck is mechanically irritated — by joint dysfunction, poor posture, or muscle tension — pain signals travel up that shared pathway and your brain interprets them as a headache.
In other words: your neck is sending pain, but your brain is feeling a headache.
This is why so many sufferers spend years on migraine medications that don't fully work. The medication is targeting brain chemistry. The actual problem is mechanical, and it sits two to three vertebrae below where anyone is looking.
How to Tell If Your Headache Is Cervicogenic
Cervicogenic headaches have specific features that distinguish them from primary headaches like true migraines or tension-type headaches. If most of these describe your experience, your neck is very likely the source:
- The pain typically starts at the base of the skull or back of the neck and spreads forward to the head, often settling behind or above one eye
- The pain is usually one-sided (though it can switch sides over time)
- The headache is provoked or worsened by neck movement — turning, looking up, looking down, or holding a position too long
- Pressure on certain points on your neck can trigger or worsen the pain
- The headache is often accompanied by neck stiffness, reduced range of motion, or a sense of tension in the upper shoulders
- Symptoms get worse after prolonged sitting, screen time, or driving
- Pain medications provide only partial or temporary relief — they take the edge off but don't eliminate the headache
- Your neurologist may have ruled out true migraine but offered no clear alternative diagnosis
If three or more of these describe what you experience, you should be evaluated specifically for a cervicogenic origin. Standard headache treatment will not resolve the underlying problem.
Why Office Workers in Muscat Are at Especially High Risk
Cervicogenic headaches are not random. They have well-documented mechanical causes — and almost all of them are amplified by modern Gulf working life.
The medical literature is direct: poor posture during work and at workstations is one of the leading causes of cervicogenic headache. Research has shown that office workers experience cervicogenic headaches at notably higher rates than other occupational groups, driven by sustained forward-head positions at computers and laptops.
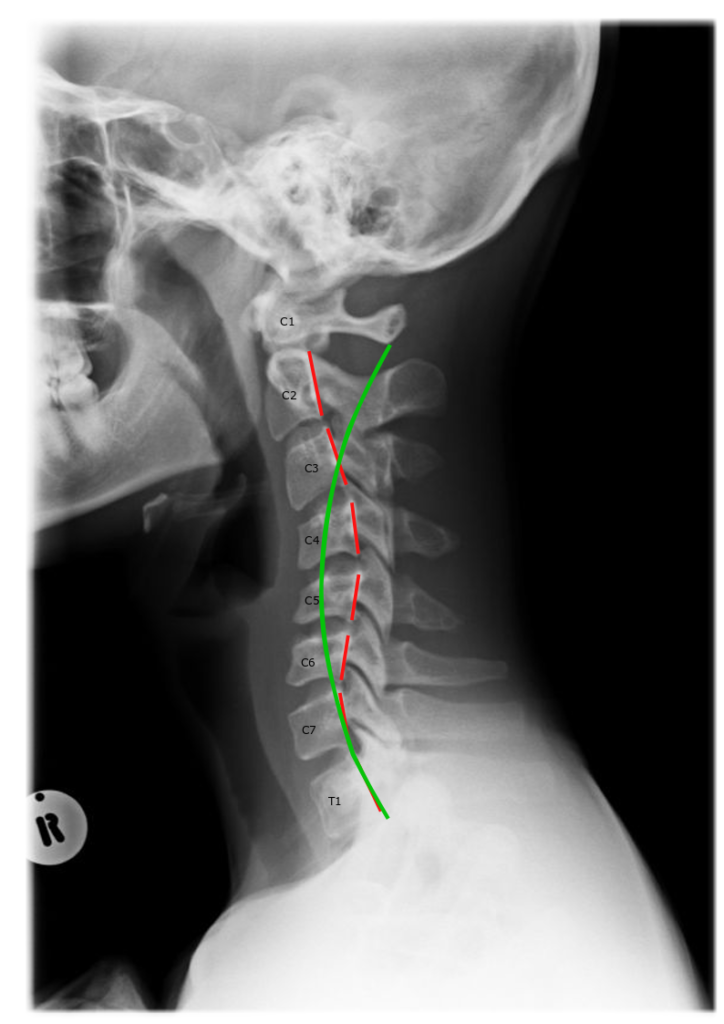
Looking down at a phone or laptop at a 60-degree angle places the equivalent of approximately 27 kilograms of force on your cervical spine — far more than the head's natural weight of 4.5 to 5.5 kilograms. Held for hours daily over years, this load gradually pulls the head forward, flattens the natural curve in your neck (the cervical lordosis), and irritates the upper cervical joints that refer pain into the head.
For Muscat-based professionals, several factors compound the problem:
- Long screen-based working days in offices in Al Khuwair, MQ, Knowledge Oasis, and across the CBD
- Long car commutes that force a forward-head, slightly tilted position for additional hours each day
- Heavy phone use during meetings, prayer-time reading, and daily life — a near-universal posture habit in the GCC
- Heat-driven indoor inactivity that eliminates the spinal mobility outdoor activity normally provides
- High caffeine consumption that masks symptoms temporarily and delays people seeking proper care
The result is a population in which chronic, recurring headaches from neck dysfunction are extraordinarily common — yet rarely identified correctly.
Why Painkillers, Massage, and Generic Physiotherapy Don't Fix It
The standard pathway for headache sufferers in Muscat usually looks like this: pharmacy painkillers, then prescription medication from a GP, then a neurologist consultation, then perhaps a few sessions of generic physiotherapy or massage. Each of these has a role — but none of them addresses the actual cause when the headache is cervicogenic.
Painkillers mask pain. They do nothing to correct the mechanical dysfunction in your neck. Worse, frequent painkiller use over months can cause medication overuse headache — a separate, additional headache that develops because of the medication itself. Research from the broader Middle East region has identified medication overuse headache as one of the most common secondary headaches in our population.
Migraine medications target brain-level chemistry. If your headache is actually coming from the upper cervical joints, no amount of triptans or beta-blockers will eliminate the source. They may reduce symptom intensity, but the headache returns the moment medication wears off.
Massage and generic physiotherapy reduce muscle tension temporarily. Massage feels excellent, and there is real value in releasing tight upper trapezius and suboccipital muscles. But if the underlying cervical curve has flattened or reversed — which is common in chronic sufferers — soft tissue work alone cannot restore the structural alignment that's causing the joints to refer pain.
Manual chiropractic adjustments can provide meaningful short-term relief by improving joint mobility. However, traditional chiropractic typically focuses on symptom relief through adjustments rather than measurable correction of cervical alignment over time.
The pattern across all of these is the same: each treats the symptom effectively for a while, but none addresses the structural cause — which is where chronic cases need to be treated for lasting resolution.
The CBP Difference: Correcting the Cause, Not Just the Symptom
This is where our approach at CBP Precision Spine Center diverges from standard care. We specialize in Chiropractic BioPhysics® (CBP) — the most heavily researched chiropractic technique in the world, supported by over 200 peer-reviewed studies, with multiple published case studies specifically documenting resolution of chronic headaches and migraines through cervical curve restoration.
The principle is straightforward: if the source of your headache is a flattened or reversed cervical curve combined with forward-head posture, the only durable solution is to physically restore that curve. Soft tissue work, painkillers, and standard adjustments cannot do this. Structured, measured cervical correction can.
CBP treatment for cervicogenic headache typically combines:
1. Objective diagnostic imaging. We measure your cervical curve precisely using digital X-ray. We don't guess at what your spine looks like — we image it, measure the angles, and document exactly how much it has shifted from ideal alignment. Without this baseline, no treatment can be tracked for real progress.
2. Mirror-image cervical adjustments. Rather than generic adjustments, CBP applies forces in the precise direction opposite to your specific misalignment pattern.
3. Cervical extension traction. This is the cornerstone of curve restoration. Calibrated traction is applied to physically pull your cervical spine back toward its ideal lordotic shape over a series of sessions.
4. Targeted corrective exercises. Specific home exercises are prescribed based on your spinal pattern, not generic neck stretches that may help one patient and worsen another.
5. Postural retraining tools. This is where dedicated tools like the Cervigard FHP Correction Collar become valuable — but more on that below.
The published research is striking. CBP case studies have documented full resolution of chronic migraines and decade-long headaches in patients whose cervical curves were restored through this protocol. One published case showed complete recovery from chronic migraines and neck pain after twelve weeks of treatment, with the correction maintained at long-term follow-up.
How Cervigard Supports Cervical Curve Recovery at Home
One of the most important advances in postural correction in recent years has been the development of structured home tools that work alongside in-clinic CBP treatment. The Cervigard FHP Correction Collar is among the most clinically meaningful of these.
Cervigard is specifically designed to address forward head posture (FHP) — the postural pattern caused by years of looking down at phones, laptops, and computer screens. The collar applies a precise corrective force that helps restore the cervical curve, with a recommended protocol of approximately 20 minutes of daily use over a minimum six-week initial correction phase, followed by maintenance use a few times per week.
For patients with cervicogenic headaches in Muscat, Cervigard becomes a powerful complement to in-clinic care. While CBP cervical extension traction during your appointments delivers the primary corrective force, daily Cervigard use at home reinforces that correction between sessions. For office workers, professionals who travel frequently, or anyone who cannot attend in-clinic care multiple times per week, this combination dramatically accelerates results.
It is important to be clear: a correction collar alone, without a proper postural assessment and integrated CBP protocol, is not a complete solution. Like any structural correction tool, Cervigard works best as part of a measured, professionally guided plan — not as a self-prescribed device. We assess each patient individually before recommending it, and we provide detailed protocols on how and when to use it for maximum benefit.
What Recovery Actually Looks Like
When a patient with chronic cervicogenic headaches comes to our clinic in Azaiba, the process is structured and measured:
Weeks 1–2: Comprehensive assessment, digital cervical imaging, postural analysis, and the development of a personalized correction plan. Patients often experience some symptom relief during this period simply from the initial adjustments and education about posture habits.
Weeks 3–12: The active correction phase. Two to three in-clinic sessions per week combining mirror-image adjustments, calibrated cervical extension traction, and corrective exercises. Cervigard or similar home tools may be introduced once postural mechanics are established. Most patients experience significant reduction in headache frequency and intensity during this phase — often dropping from daily headaches to occasional ones.
Months 4–6: Stabilization. Re-imaging confirms structural change. Treatment frequency reduces. The focus shifts to locking in correction and preventing return of the original pattern.
Ongoing: Periodic maintenance to preserve correction long-term. Published research shows that without maintenance, some loss of correction is common — but the structural improvements achieved during active care remain substantially better than the starting point even years later.
The honest truth: chronic cervicogenic headaches developed over years cannot be fixed in a week. But the trajectory is consistent — patients who commit to a measured, imaging-based correction protocol typically report 70 to 100 percent reduction in headache burden, and many experience full resolution.
When You Should Be Evaluated
Book a cervical assessment if any of the following apply to you:
- You experience headaches more than four days per month
- Your headache pain begins at or refers from the back of the neck or base of the skull
- Painkillers and migraine medications only partially help
- Your headaches are clearly worsened by computer work, phone use, or driving
- You have been diagnosed with migraine but the diagnosis "doesn't quite fit"
- You experience neck stiffness alongside your headaches
- Headaches are interfering with your work, sleep, or quality of life
A proper cervical assessment is straightforward, non-invasive, and gives you something most headache sufferers in Muscat have never received: an objective measurement of whether your neck is the actual source of your pain. If it is, there is a clear, evidence-based path forward.
You Don't Have to Live With This
Chronic headaches and migraines wear people down in ways that are difficult to describe to anyone who hasn't experienced them. Days lost to dark rooms. Family events missed. Productivity halved. The constant, low-grade fear of when the next one will hit.
If you've been told it's just migraine, or just tension, or just stress — and treatment hasn't given you your life back — there is another diagnosis worth investigating. Cervicogenic headache is treatable. The cervical curve is correctable. The pain pathway is interruptible. And the research supporting structural correction through CBP is strong.
We are the first certified Chiropractic BioPhysics® (CBP) clinic in the region, and we treat cervicogenic headache cases regularly — including patients who have spent years on the standard headache pathway with limited results.
Book your cervical assessment today — and finally find out whether your headaches have been coming from somewhere no one has thought to check.
صداعٌ مزمن أو نصفي لا يتوقّف؟ قد يكون مصدره رقبتك. اكتشف علاج صداع المنشأ العنقي في مسقط في مركز CBP للدقة في العمود الفقري.
الصداع الذي يُغفله معظم الأطباء
لقد جرّبتَ كلّ شيء. الباراسيتامول. مُسكِّناتٍ أقوى من الصيدلية. ربّما موعداً مع أخصائي أعصاب انتهى بتشخيص "صداعٌ توتّري" أو "صداعٌ نصفي" ووصفةٍ طبية تنفع لساعاتٍ قليلة. امتنعتَ عن الكافيين. تتبّعتَ مُحفّزات الطعام. نمتَ أكثر، نمتَ أقلّ، شربتَ ماءً أكثر، جلستَ في غرفٍ مُعتمة.
ومع ذلك، يستمرّ الصداع. يومان، ثلاثة، أحياناً خمسة أيام في الأسبوع. يبدأ من قاعدة الجمجمة، يتسلّق إلى مؤخّرة الرأس، ويستقرّ خلف إحدى العينين. يشتدّ حين تجلس على مكتبك طويلاً. يشتدّ حين تنظر إلى هاتفك. يشتدّ حين تُدير رأسك بطريقةٍ معيّنة.
إن كان هذا يبدو مألوفاً، فثمّة احتمالٌ كبير جداً أنّ ما تُعانيه ليس صداعاً نصفياً على الإطلاق. إنّه صداع المنشأ العنقي — صداعٌ ينشأ في الرقبة، لا في الدماغ. ويُمثّل ما يُقدَّر بـ 15 إلى 20 بالمئة من جميع حالات الصداع المزمن، مع تأثرٍ غير متناسب لدى موظفي المكاتب.
في الشرق الأوسط تحديداً، وجدت أبحاثٌ حديثة أنّ 35.5% من المرضى الذين يُراجعون بسبب الصداع يُعانون فعلياً من صداعٍ ثانوي — أي صداعٍ ناتجٍ عن مشكلةٍ أخرى في الجسم، ويُعدّ صداع المنشأ العنقي من أكثر أنواعه شيوعاً. أي ما يقرب من واحدٍ من كلّ ثلاثة. ومع ذلك، يقضي معظم المرضى في مسقط سنواتٍ قبل أن يفحص أحدٌ رقبتهم بوصفها مصدراً محتملاً.
تُوضّح هذه المقالة لماذا يحدث ذلك، وكيف تُميّز بين الصداع النصفي الحقيقي والصداع القادم من رقبتك، وما الذي يُجدي فعلاً في علاجه.
ما هو صداع المنشأ العنقي بالضبط؟
التعريف الطبي دقيق. صداع المنشأ العنقي هو صداعٌ يَنتج عن اضطرابٍ في العمود الفقري العنقي — الفقرات السبع في رقبتك — أو الأنسجة الرخوة المحيطة بها. يبدأ الألم في الرقبة أو قاعدة الجمجمة وينتقل صعوداً إلى الرأس، وكثيراً ما يظهر بطرقٍ تُشبه الصداع النصفي أو التوتّري تماماً.
الآلية مفهومةٌ جيداً. الأعصاب القادمة من الفقرات العنقية العلوية (تحديداً C1 إلى C3) تتشارك مساراً مع العصب الثلاثي التوائم في ما يُعرف بالنواة الثلاثية العنقية (Trigeminal-Cervical Nucleus). فحين تتعرّض الرقبة العلوية لتهيّجٍ ميكانيكي — بسبب اختلال المفاصل، أو الوضعية الخاطئة، أو توتّر العضلات — تنتقل إشارات الألم عبر هذا المسار المشترك، فيُفسّرها دماغك على أنّها صداع.
بعبارةٍ أخرى: رقبتك تُرسل ألماً، ودماغك يشعر بصداع.
ولهذا يقضي كثيرٌ من المرضى سنواتٍ على أدوية الصداع النصفي دون نتائج كاملة. الدواء يستهدف كيمياء الدماغ. أمّا المشكلة الحقيقية فميكانيكية، وموقعها فقرتان أو ثلاث أسفلَ المكان الذي يبحث فيه الجميع.
كيف تعرف أنّ صداعك من منشأٍ عنقي؟
لصداع المنشأ العنقي ملامح محدّدة تُميّزه عن الصداع الأوّلي مثل الصداع النصفي الحقيقي أو صداع التوتّر. إن وصفتْ معظم هذه النقاط تجربتك، فمن المُرجَّح جداً أنّ رقبتك هي المصدر:
- يبدأ الألم عادةً من قاعدة الجمجمة أو مؤخّرة الرقبة ثم ينتشر إلى الأمام نحو الرأس، ويستقرّ غالباً خلف إحدى العينين أو فوقها
- الألم في الغالب في جانبٍ واحد (وإن كان قد يتنقّل بين الجانبين بمرور الوقت)
- الصداع يُحفَّز أو يشتدّ بحركة الرقبة — كالالتفات، أو النظر إلى الأعلى، أو إلى الأسفل، أو الثبات في وضعيةٍ واحدة طويلاً
- الضغط على نقاطٍ معيّنة في رقبتك قد يُحفِّز الألم أو يُفاقمه
- يُصاحب الصداع غالباً تيبّسٌ في الرقبة، أو محدوديةٌ في نطاق الحركة، أو شعورٌ بالشدّ في أعلى الكتفين
- تشتدّ الأعراض بعد الجلوس المطوّل، أو وقت الشاشة، أو القيادة
- مُسكِّنات الألم تُقدّم راحةً جزئية أو مؤقتة فقط — تُخفّف حدّته دون أن تُلغيه
- ربّما يكون أخصائي الأعصاب قد استبعدَ الصداع النصفي الحقيقي دون تقديم تشخيصٍ بديلٍ واضح
إن وصفت ثلاثٌ من هذه النقاط أو أكثر تجربتك، فينبغي تقييمك تحديداً للبحث عن منشأٍ عنقي. فالعلاج المعتاد للصداع لن يُعالج المشكلة الكامنة.
لماذا يكون موظفو المكاتب في مسقط مُعرَّضين بشكلٍ خاص؟
صداع المنشأ العنقي ليس عشوائياً. له أسبابٌ ميكانيكيةٌ موثّقةٌ جيداً — وكلّها تقريباً تتفاقم بسبب الحياة العملية الحديثة في الخليج.
الأدبيّات الطبية صريحة: الوضعية الخاطئة أثناء العمل وعند محطّات العمل من الأسباب الرئيسية لصداع المنشأ العنقي. وقد أظهرت الأبحاث أنّ موظفي المكاتب يُعانون من صداع المنشأ العنقي بمعدّلاتٍ أعلى ملحوظاً من المهن الأخرى، نتيجة الوضعيات المُستمرّة لانحناء الرأس إلى الأمام أمام الكمبيوتر واللابتوب.
النظر إلى هاتف أو لابتوب بزاوية 60 درجة يُولّد على عمودك الفقري العنقي قوّةً تُعادل تقريباً 27 كيلوغراماً — أي أكثر بكثير من الوزن الطبيعي للرأس البالغ 4.5 إلى 5.5 كيلوغرام. وحين يُحمَل هذا الثقل ساعاتٍ يومياً على مدى سنوات، فإنّه يسحب الرأس إلى الأمام تدريجياً، ويُسطِّح الانحناء الطبيعي للرقبة (الانحناء العنقي القعسي / Cervical Lordosis)، ويُهيِّج المفاصل العنقية العليا التي تُحيل الألم إلى الرأس.
بالنسبة للمهنيين في مسقط، تتضافر عدّة عوامل لتُفاقم المشكلة:
- أيام عملٍ طويلة أمام الشاشات في مكاتب الخوير، ومدينة السلطان قابوس، وواحة المعرفة، وأنحاء منطقة الأعمال المركزية
- تنقّلاتٌ طويلة بالسيارة تفرض وضعيةَ رأسٍ مُنحنياً إلى الأمام ومائلٍ قليلاً لساعاتٍ إضافية يومياً
- استخدامٌ مكثّف للهاتف خلال الاجتماعات، والقراءة في أوقات الصلاة، والحياة اليومية — وهي عادةُ وضعيةٍ شبه عامة في الخليج
- خمولٌ داخلي ناتج عن الحرارة يُلغي الحركة الطبيعية للعمود الفقري التي يُتيحها النشاط الخارجي عادةً
- استهلاكٌ عالٍ للكافيين يُخفي الأعراض مؤقتاً ويُؤخّر اللجوء إلى رعايةٍ مناسبة
والنتيجة: شريحةٌ سكّانية يكون فيها الصداع المزمن المُتكرّر الناتج عن خللٍ في الرقبة شائعاً بشكلٍ استثنائي — ومع ذلك نادراً ما يُشخَّص تشخيصاً صحيحاً.
لماذا لا تُجدي المُسكِّنات والتدليك والعلاج الطبيعي العام نفعاً؟
المسار المعتاد لمن يُعاني من الصداع في مسقط يبدو في الغالب هكذا: مسكّناتٌ من الصيدلية، ثم وصفةٌ طبية من طبيبٍ عام، ثم استشارة أخصائي أعصاب، ثم ربّما بضع جلساتٍ من العلاج الطبيعي العام أو التدليك. ولكلٍّ من هذه دور — ولكنّ أيّاً منها لا يُعالج السبب الفعلي حين يكون الصداع من منشأٍ عنقي.
المُسكِّنات تُخفي الألم. ولا تُجدي شيئاً في تصحيح الخلل الميكانيكي في رقبتك. والأسوأ أنّ الاستخدام المتكرّر للمُسكِّنات على مدى أشهر قد يُسبّب صداعاً ناتجاً عن الإفراط في تناول الأدوية (Medication Overuse Headache) — وهو صداعٌ منفصلٌ وإضافي يتطوّر بسبب الدواء نفسه. وقد حدّدت الأبحاث في منطقة الشرق الأوسط الموسّعة هذا النوع باعتباره من أكثر أنواع الصداع الثانوي شيوعاً في مجتمعنا.
أدوية الصداع النصفي تستهدف كيمياء الدماغ. فإن كان صداعك قادماً فعلياً من المفاصل العنقية العليا، فلن تُلغي مصدر الألم أيّ كميةٍ من التريبتانات أو حاصرات بيتا. قد تُقلّل شدّة الأعراض، لكنّ الصداع يعود فور زوال مفعول الدواء.
التدليك والعلاج الطبيعي العام يُخفّفان توتّر العضلات مؤقتاً. والتدليك يبعث على الراحة، ولإرخاء العضلات الشبه منحرفة العلوية والعضلات تحت القذالية المتوتّرة قيمةٌ حقيقية. ولكن إن كان الانحناء العنقي قد تسطّح أو انعكس — وهذا شائعٌ في الحالات المزمنة — فإنّ العمل على الأنسجة الرخوة وحده لا يستطيع استعادة المحاذاة البنيوية التي تجعل المفاصل تُحيل الألم.
التعديلات اليدوية في تقويم العمود الفقري التقليدي قد تُقدّم راحةً ملحوظةً قصيرة المدى عبر تحسين حركة المفاصل. لكنّ التقويم التقليدي يُركّز عادةً على تخفيف الأعراض من خلال التعديلات، لا على التصحيح القابل للقياس للمحاذاة العنقية عبر الزمن.
النمط في كلّ ذلك واحد: كلٌّ منها يُعالج العَرَض بفعاليةٍ لفترة، لكنّ أيّاً منها لا يُعالج السبب البنيوي — وهنا تحتاج الحالات المزمنة إلى علاجٍ يُحقّق نتائج دائمة.
الفرق في CBP: علاج السبب، لا مجرّد العَرَض
هنا يَختلف نهجنا في مركز CBP للدقة في العمود الفقري عن الرعاية المعتادة. نحن متخصّصون في Chiropractic BioPhysics® (CBP) — أكثر تقنيات تقويم العمود الفقري التي خضعت للبحث في العالم، وتدعمها أكثر من 200 دراسة محكَّمة، مع دراسات حالة منشورة عديدة توثّق تحديداً زوال الصداع المزمن والصداع النصفي من خلال استعادة الانحناء العنقي.
المبدأ بسيط: إن كان مصدر صداعك انحناءً عنقياً مُسطّحاً أو معكوساً مع وضعية رأسٍ منحنية إلى الأمام، فإنّ الحلّ الدائم الوحيد هو الاستعادة الفيزيائية لذلك الانحناء. والعمل على الأنسجة الرخوة، والمُسكِّنات، والتعديلات المعتادة لا تستطيع تحقيق ذلك. أمّا التصحيح العنقي المُنظَّم والقابل للقياس فيستطيع.
يجمع علاج CBP لصداع المنشأ العنقي عادةً بين:
1. تصويرٌ تشخيصيٌّ موضوعي. نقيس انحناء فقراتك العنقية بدقّة باستخدام الأشعة السينية الرقمية. لا نُخمّن شكل عمودك الفقري — بل نُصوّره، ونقيس الزوايا، ونوثّق بالضبط مقدار انحرافه عن المحاذاة المثالية. وبدون هذا الأساس، لا يمكن تتبّع تقدّم العلاج بصدق.
2. تعديلات الصورة المرآوية العنقية (Mirror-Image Cervical Adjustments). بدلاً من التعديلات العامة، تُطبّق CBP قوى في الاتجاه الدقيق المعاكس لنمط الانحراف الخاصّ بك.
3. شدّ التمدّد العنقي (Cervical Extension Traction). هذا هو حجر الزاوية في استعادة الانحناء. يُطبَّق شدٌّ مُعايَر لسحب فقراتك العنقية فيزيائياً نحو شكلها القعسي المثالي عبر سلسلةٍ من الجلسات.
4. تمارين تصحيحية مُستهدَفة. تُوصَف تمارين منزلية محدّدة بناءً على نمطك العمودي، لا تمارين رقبةٍ عامة قد تُساعد مريضاً وتُؤذي آخر.
5. أدوات إعادة تدريب الوضعية. هنا تُصبح أدواتٌ مُخصّصة مثل طوق Cervigard لتصحيح وضعية الرأس الأمامية ذات قيمةٍ حقيقية — وسنتحدّث عنها بمزيدٍ من التفصيل أدناه.
الأبحاث المنشورة لافتة. وثّقت دراسات حالة CBP زوالاً كاملاً للصداع النصفي المزمن وللصداع الذي استمرّ لعقود، لدى مرضى استُعيدت لديهم الانحناءات العنقية من خلال هذا البروتوكول. أظهرت إحدى الحالات المنشورة تعافياً كاملاً من الصداع النصفي المزمن وآلام الرقبة بعد اثني عشر أسبوعاً من العلاج، مع الحفاظ على التصحيح في المتابعة طويلة المدى.
كيف يدعم Cervigard استعادة الانحناء العنقي في المنزل؟
من أهمّ التطوّرات في مجال تصحيح الوضعية في السنوات الأخيرة تطوير أدواتٍ منزلية مُنظَّمة تعمل جنباً إلى جنب مع علاج CBP داخل العيادة. ويُعدّ طوق Cervigard لتصحيح وضعية الرأس الأمامية (FHP Correction Collar) من أكثرها أهميةً سريرياً.
صُمِّم Cervigard خصيصاً لمعالجة وضعية الرأس الأمامية (Forward Head Posture) — النمط الوضعي الناتج عن سنواتٍ من النظر إلى الهواتف، واللابتوبات، وشاشات الكمبيوتر إلى الأسفل. يُطبّق الطوق قوّةً تصحيحيةً دقيقة تُساعد على استعادة الانحناء العنقي، ضمن بروتوكولٍ مُوصى به يبلغ نحو 20 دقيقةً يومياً على مدى مرحلة تصحيحٍ أوّلية لا تقلّ عن ستة أسابيع، تليها استخدامٌ مستمرٌّ بضع مرّاتٍ في الأسبوع للحفاظ على النتائج.
بالنسبة لمرضى صداع المنشأ العنقي في مسقط، يُصبح Cervigard تكملةً قويةً للرعاية داخل العيادة. ففي حين يُقدّم شدّ التمدّد العنقي في CBP خلال مواعيدك القوّةَ التصحيحية الرئيسية، يُعزّز استخدام Cervigard اليومي في المنزل ذلك التصحيح بين الجلسات. وبالنسبة لموظفي المكاتب، أو المهنيين الذين يُسافرون كثيراً، أو لكلّ من لا يستطيع حضور رعايةٍ داخل العيادة عدّة مرّاتٍ في الأسبوع، يُسرِّع هذا الجمع النتائج تسريعاً ملحوظاً.
من المهمّ التوضيح: طوق التصحيح بمفرده، دون تقييمٍ وضعيٍّ مناسبٍ وبروتوكول CBP المتكامل، ليس حلاً كاملاً. فمثل أيّ أداة تصحيحٍ بنيوية، يعمل Cervigard بأفضل صورته كجزءٍ من خطّةٍ مُقاسة وموجَّهة مهنياً — لا كأداةٍ يصفها المريض لنفسه. نحن نُقيِّم كلّ مريضٍ على حدة قبل التوصية بها، ونُقدّم بروتوكولات مفصّلة حول كيفية وأوقات استخدامها لتحقيق أقصى فائدة.
كيف يبدو التعافي فعلياً؟
حين يأتي مريضٌ يُعاني من صداع المنشأ العنقي المزمن إلى عيادتنا في العذيبة، تكون العملية مُنظَّمة وقابلة للقياس:
الأسبوعان 1–2: تقييمٌ شامل، وتصويرٌ رقمي للفقرات العنقية، وتحليلٌ للوضعية، وبناءُ خطّة تصحيحٍ شخصية. يشعر المرضى غالباً ببعض الراحة من الأعراض خلال هذه الفترة بفعل التعديلات الأوّلية والتثقيف حول عادات الوضعية.
الأسابيع 3–12: مرحلة التصحيح النشط. جلستان إلى ثلاث في العيادة أسبوعياً تجمع بين تعديلات الصورة المرآوية، وشدّ التمدّد العنقي المُعايَر، والتمارين التصحيحية. وقد يُدخَل Cervigard أو أدواتٌ منزليةٌ مماثلة بمجرّد ترسيخ الميكانيكا الوضعية. يشهد معظم المرضى انخفاضاً ملحوظاً في تكرار الصداع وشدّته خلال هذه المرحلة — وكثيراً ما ينتقلون من صداعٍ يومي إلى صداعٍ متفرّق.
الأشهر 4–6: التثبيت. تُؤكّد إعادة التصوير التغيّر البنيوي. تنخفض وتيرة العلاج. ويتحوّل التركيز إلى ترسيخ التصحيح ومنع عودة النمط الأصلي.
المتابعة المستمرّة: صيانةٌ دوريةٌ للحفاظ على التصحيح طويل المدى. تُظهر الأبحاث المنشورة أنّه دون صيانة، يكون فقدان جزءٍ من التصحيح أمراً شائعاً — لكنّ التحسّنات البنيوية المُحقَّقة خلال الرعاية النشطة تظلّ أفضل بشكلٍ كبيرٍ من نقطة البداية حتى بعد سنوات.
الحقيقة الصريحة: صداع المنشأ العنقي المزمن الذي تطوّر على مدى سنوات لا يمكن إصلاحه في أسبوع. لكنّ المسار ثابت — المرضى الذين يلتزمون ببروتوكول تصحيحٍ مُقاسٍ يستند إلى التصوير يُبلِّغون عادةً عن انخفاضٍ في عبء الصداع بنسبة 70 إلى 100 بالمئة، ويختبر كثيرون منهم تعافياً كاملاً.
متى ينبغي عليك إجراء التقييم؟
احجز تقييماً للفقرات العنقية إذا انطبق عليك أيٌّ ممّا يلي:
- تُعاني من صداعٍ أكثر من أربعة أيامٍ في الشهر
- يبدأ ألم الصداع لديك من مؤخّرة الرقبة أو قاعدة الجمجمة، أو يُحال منهما
- المُسكِّنات وأدوية الصداع النصفي تُساعد جزئياً فقط
- يتفاقم صداعك بوضوح بفعل العمل على الكمبيوتر، أو استخدام الهاتف، أو القيادة
- تمّ تشخيصك بالصداع النصفي لكنّ التشخيص "لا يبدو ملائماً تماماً"
- تُعاني من تيبّسٍ في الرقبة مع الصداع
- يُعرقل الصداع عملك، أو نومك، أو جودة حياتك
تقييم الفقرات العنقية المناسب بسيط، وغير اقتحامي، ويُقدّم لك ما لم يحصل عليه معظم مرضى الصداع في مسقط: قياسٌ موضوعي لمعرفة ما إذا كانت رقبتك هي المصدر الفعلي لألمك. وإن كانت كذلك، فثمّة طريقٌ واضح ومدعوم بالأدلة للأمام.
لستَ مُجبَراً على التعايش مع هذا
الصداع المزمن والصداع النصفي يُنهكان الناس بطرقٍ يصعب وصفها لمن لم يَختبرها. أيامٌ تُهدَر في غرفٍ مُعتمة. مناسباتٌ عائلية فائتة. إنتاجيةٌ مُنصَّفة. والخوف الدائم منخفض الشدة من موعد النوبة التالية.
إن قيل لك إنّه مجرّد صداعٍ نصفي، أو مجرّد توتّر، أو مجرّد ضغطٍ نفسي — ولم تُعِد إليك المعالجة حياتك — فثمّة تشخيصٌ آخر يستحقّ الاستقصاء. صداع المنشأ العنقي قابلٌ للعلاج. والانحناء العنقي قابلٌ للتصحيح. ومسار الألم قابلٌ للقطع. والأبحاث الداعمة للتصحيح البنيوي عبر CBP قويّة.
نحن أول عيادة معتمدة في تقنية Chiropractic BioPhysics® (CBP) في المنطقة، ونُعالج حالات صداع المنشأ العنقي بانتظام — بمن فيهم المرضى الذين أمضوا سنواتٍ على المسار المعتاد للصداع بنتائج محدودة.
احجز تقييم فقراتك العنقية اليوم — واكتشف أخيراً ما إذا كان صداعك يأتي من مكانٍ لم يُفكّر أحدٌ في فحصه.
سلطنة عمان - مسقط - العذيبة
شارع 18 نوفمبر - فيلا 336