Diagnosed with a slipped disc in Muscat? International guidelines recommend conservative care first. Discover non-surgical disc treatment at CBP Precision Spine.
A Diagnosis That Doesn't Have to End in the Operating Room
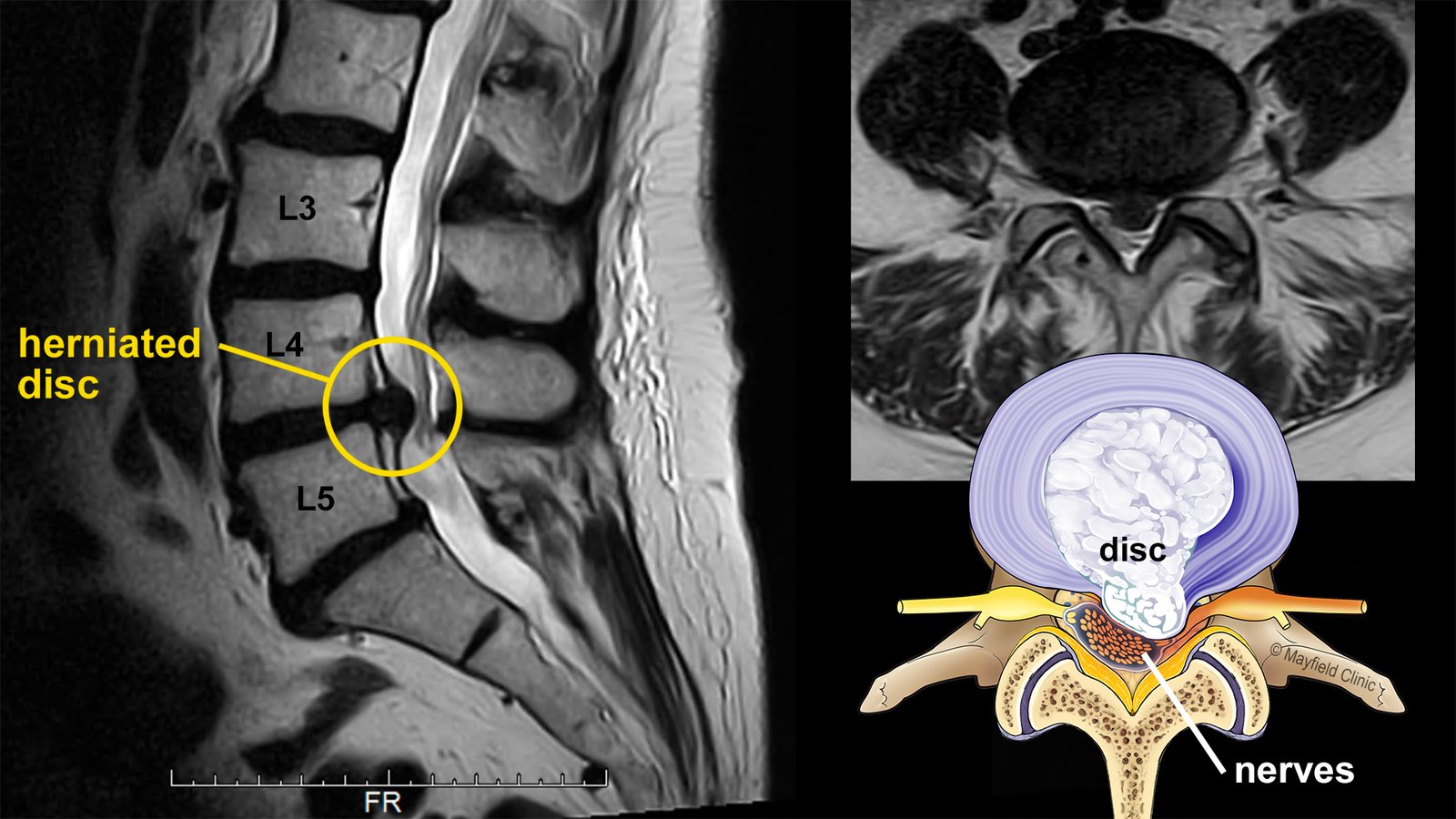
You've had the MRI. You've sat across from a doctor who pointed to a dark spot on the scan and said the words: herniated disc, or slipped disc, or prolapsed disc. Maybe they followed it with a referral to a spinal surgeon. Maybe they mentioned a discectomy or a fusion. Maybe you went home convinced surgery was inevitable.
If you're searching for answers right now — typing "slipped disc Muscat," "herniated disc treatment Oman," or "disc surgery alternatives" into Google late at night — you are not alone. And you may not have been told the most important fact about your diagnosis.
According to international clinical guidelines published by the World Federation of Neurosurgical Societies (WFNS) Spine Committee, conservative (non-surgical) care is the recommended first-line treatment for lumbar disc herniation in patients who do not have specific red-flag neurological deficits. This recommendation comes from neurosurgeons themselves. They are not anti-surgery. They are pro-evidence — and the evidence is clear.
The evidence is also striking in another way: more than 85% of patients with acute disc herniation and nerve pain will have their symptoms resolve over time with appropriate conservative care. And in over half of cases, the herniated disc material itself partially or fully reabsorbs into the body — meaning the visible bulge on your MRI can shrink on its own, given the right conditions.
This article explains what your slipped disc actually is, what international guidelines actually recommend, when surgery genuinely is necessary, and what conservative treatment looks like at our CBP Precision Spine Center clinic in Muscat.
What "Slipped Disc" Actually Means
The term "slipped disc" is a useful shorthand, but it's slightly misleading. Discs don't slip out of place. The intervertebral discs sitting between each pair of spinal vertebrae are firmly anchored. What actually happens is more specific — and understanding it changes how you think about treatment.
Each disc has two parts: a tough outer ring (the annulus fibrosus) and a soft, gel-like inner core (the nucleus pulposus). When the outer ring weakens or tears, the inner core can push outward through the weakened wall. Depending on how far it pushes, doctors describe this as:
- Disc bulge — mild outward pressure on the disc wall
- Disc protrusion — the inner material pushes against but does not break through the outer wall
- Disc herniation — the inner material breaks through the outer wall
- Disc extrusion or sequestration — material has separated and migrated away from the disc
When this displaced material presses on a nearby nerve root — most commonly in the lower back, irritating the sciatic nerve — the result is pain that radiates down the leg, often with tingling, numbness, or weakness. This combination of disc problem plus nerve irritation is what many people describe simply as "slipped disc pain," and clinically it's known as lumbar radiculopathy or, more familiarly, sciatica.
What International Guidelines Actually Recommend
This is the part most patients in Muscat are never properly told.
The World Federation of Neurosurgical Societies Spine Committee is one of the most authoritative international bodies on spinal care. Their official recommendation for lumbar disc herniation is direct: "Conservative treatment is recommended as the first-line treatment for LDH in patients who do not have neurologic deficits such as motor deficits or cauda equina syndrome."
The North American Spine Society (NASS) 2022 clinical guidelines echo the same position: surgery is indicated only for patients with significant or progressive neurological impairment, intractable pain that has not responded to conservative care, or specific structural abnormalities that require surgical correction.
The standard conservative trial period before surgery is even considered is 4 to 6 weeks, and in many guidelines, up to 8 weeks. During this period, the data shows that:
- More than 85% of acute disc herniation cases with radiculopathy resolve over time with appropriate non-surgical care
- Spontaneous reabsorption of the herniated disc material occurs in over half of symptomatic cases managed conservatively — meaning your body can, under the right conditions, reabsorb the disc material that's currently causing your pain
- Surgery is not the default first option. It is the option reserved for cases where conservative care has been given a fair trial and has failed, or where specific red flags are present from the start
What this means in practical terms: if you have been recently diagnosed with a slipped disc and you do not have the specific red-flag symptoms listed below, the clinically appropriate first step — according to the surgeons' own international guidelines — is a structured course of conservative care. Not an immediate operation.
When Surgery Is Genuinely Necessary — The Red Flags You Cannot Ignore
This article is not anti-surgery. Surgery saves people. There are specific situations where surgical intervention is not only appropriate but urgent. If any of the following apply to you, stop reading and seek emergency medical evaluation immediately:
- Cauda equina syndrome symptoms: loss of bladder or bowel control, numbness in the saddle/groin area, or sudden severe weakness in both legs
- Progressive neurological deficit: worsening weakness in a leg or foot (foot drop, inability to lift the foot, severe muscle wasting)
- Severe, intractable pain that is not responding at all to any conservative measure and is escalating rapidly
- Sudden loss of reflexes or sensation in a clear pattern matching a specific nerve root
These are clear surgical indications, and any responsible clinician — including us — will refer you immediately to a spinal surgeon if these are present. The orthopedic surgeons and neurosurgeons at hospitals like Apollo, Muscat Private Hospital, and Royal Hospital are skilled professionals, and we work alongside their referral pathways when surgery is genuinely indicated.
What this article is about is the much larger group of slipped disc patients — perhaps 80 to 90 percent of all cases — who do not have these red flags, who have been told they "may need surgery," and who deserve to know that the international guidelines say conservative care should come first.
Why Many Disc Herniation Patients Reabsorb Without Surgery
The fact that a herniated disc can shrink and reabsorb on its own surprises most patients. It surprises some clinicians too. But it is well-documented in the medical literature.
When the inner disc material pushes through the outer wall, the body recognizes the displaced material as something that doesn't belong outside the disc capsule. Inflammatory cells move in and gradually break down the protruding material — a natural reabsorption process. Studies show this happens in more than half of symptomatic cases managed conservatively, with larger herniations actually showing higher rates of reabsorption than smaller ones in some research.
For reabsorption to occur, two conditions help significantly:
- Reduced mechanical pressure on the affected disc — achieved through proper spinal alignment, decompression, and avoidance of postures that compress the herniation further
- Reduced local inflammation around the nerve root — managed through inflammation control, targeted therapies, and progressive movement restoration
This is exactly what a properly designed conservative care program is engineered to provide. It is not passive waiting. It is active creation of the conditions in which your body's natural healing processes can succeed.
What Conservative Care Should Actually Include
Not all conservative care is equal. A patient who is told to "rest, take painkillers, and come back in a month" is not receiving evidence-based conservative treatment. They are being told to wait — which is different.
A proper conservative care program for slipped disc, based on international guidelines and clinical evidence, should include:
1. Objective diagnostic assessment. Detailed history, physical examination, neurological testing, and review of imaging. The goal is to identify exactly which disc level is involved, which nerve root is affected, and whether any red flags require immediate surgical referral.
2. Pain and inflammation management. Where appropriate, this can include short-term anti-inflammatory medication, ice/heat protocols, and targeted modalities. The goal is to reduce inflammation around the nerve root, not to mask pain indefinitely with painkillers.
3. Mechanical decompression. This is critical and often missing from generic physiotherapy. Properly applied lumbar traction and decompression can reduce pressure on the affected disc, creating the mechanical conditions that support natural reabsorption.
4. Postural and structural correction. A herniated disc rarely occurs on a perfectly aligned spine. The vast majority of disc patients have years of accumulated postural dysfunction — flattened lumbar curves, anterior pelvic tilt, weakened core, or compensatory shifts — that placed unequal load on the disc until it failed. Without correcting that underlying alignment, even a fully reabsorbed disc is at high risk of re-injury.
5. Targeted soft tissue and muscle therapy. Where chronic muscle spasm and fascial restriction are contributing to the pain pattern, extracorporeal shockwave therapy can be valuable. Shockwave therapy stimulates blood flow to chronic soft tissue regions and accelerates tissue repair — making it a useful addition for many slipped disc cases where surrounding musculature has become chronically tight or inflamed.
6. Progressive movement and rehabilitation. Carefully sequenced exercises designed to restore spinal stability without aggravating the disc. This is where generic YouTube exercises often fail patients — what helps one disc pattern can worsen another, and the progression must be guided.
7. Lifestyle and ergonomic adjustment. How you sit, sleep, lift, and move affects whether your disc heals or worsens. A complete care plan addresses these directly.
The CBP Method: Why Structural Correction Matters for Disc Patients
This is where the Chiropractic BioPhysics® (CBP) method offers something most conservative care programs in Muscat do not. CBP is the most heavily researched chiropractic technique in the world, supported by over 200 peer-reviewed studies. Its core principle is precise, measurable structural correction of the spine — and for slipped disc patients, this matters enormously.
Most disc herniations occur on spines that have lost their proper architecture over years. The lumbar curve has flattened. The pelvis has tilted. The vertebrae sit at angles they were never designed to sustain. Under that abnormal mechanical load, one disc eventually fails.
Generic conservative care can reduce inflammation and may even allow partial reabsorption — but if the underlying structural pattern that caused the disc to fail in the first place is not corrected, recurrence rates are high. Patients return to the same desk, the same posture, the same misalignment, and within months or years, the same level or an adjacent level fails again.
CBP treatment for slipped disc combines:
- Digital X-ray imaging to measure exactly how the spine has shifted from ideal alignment
- Mirror-image adjustments applied in the precise direction opposite to the patient's specific misalignment
- Calibrated lumbar traction and decompression to reduce pressure on the affected disc and create reabsorption-favorable conditions
- Targeted corrective exercises chosen specifically for the patient's structural pattern, not generic "back exercises"
- Where appropriate, integrated modalities including shockwave therapy and Class 4 laser therapy for inflammation control
The goal is twofold: resolve the current disc episode through conservative means where possible, and correct the underlying structural pattern so the disc does not fail again.
What Recovery Realistically Looks Like
Patients deserve honest expectations. Slipped disc recovery is not a one-week process, and we do not pretend otherwise. Here is the realistic trajectory for most non-surgical disc cases at our clinic:
Weeks 1–2: Comprehensive assessment, imaging review, and acute symptom management. The first priority is reducing inflammation around the nerve root and identifying any red flags. Most patients begin to experience some reduction in pain intensity during this period, even before structural correction has begun.
Weeks 3–8: Active treatment phase. Two to three sessions per week combining decompression traction, mirror-image adjustments, targeted modalities, and beginning rehabilitation exercises. This is the period when most patients experience meaningful symptom resolution. Following the international guidelines' 4–6 week conservative trial framework, by the end of this phase, the great majority of non-red-flag patients are substantially improved.
Months 3–6: Stabilization and structural correction phase. Treatment frequency reduces. The focus shifts to correcting the underlying postural and structural pattern that allowed the disc to fail. Re-imaging where appropriate confirms structural change.
Ongoing maintenance: Periodic check-ins to preserve correction long-term and prevent recurrence at the same or adjacent levels.
If at any point during this timeline a patient is not progressing as expected, or if red flags emerge, we refer for surgical consultation. This is not failure of conservative care — it is the responsible application of clinical guidelines, which themselves recognize that some patients do require surgery.
When You Should Book a Consultation
You should consider a conservative-care assessment at our clinic if:
- You have been recently diagnosed with a herniated disc, slipped disc, or prolapsed disc and are exploring options before surgery
- You are within the 4–8 week window since symptom onset and have not yet had a structured conservative trial
- You have leg pain, numbness, or tingling alongside lower back pain (lumbar radiculopathy / sciatica)
- You have been told you "may need surgery" but want to understand whether conservative care is appropriate first
- You have already had previous spinal surgery and want to prevent re-injury at adjacent disc levels
- You want a measurable, imaging-based assessment of your spine, not just symptom management
You should not delay a surgical evaluation if any of the red flags listed earlier are present. We will refer you immediately if they are.
A Final Word on the Surgery Decision
The decision about whether to have spinal surgery is one of the most important medical decisions a person can make. It deserves to be made with complete information.
Surgery is the right choice for some slipped disc patients — particularly those with red flags, with confirmed neurological progression, or with cases that have failed an adequate conservative trial. For those patients, modern spinal surgery in Oman is excellent and can be life-changing.
But the international guidelines are unambiguous: surgery is not the right first step for most disc herniation patients. Conservative care is. And if you are reading this article because you have been told you may need surgery, you owe it to yourself — at minimum — to understand what a properly structured conservative care program could achieve for you first.
We are the first certified Chiropractic BioPhysics® (CBP) clinic in the region, and we treat slipped disc cases regularly using internationally recognized conservative care principles. We work alongside surgical pathways when surgery is genuinely indicated, and we do not pretend conservative care is right for every case. We do, however, believe every disc patient deserves the chance to try conservative care first, the way the international guidelines recommend.
Book your slipped disc consultation today — and find out whether your case is one that could resolve without ever entering an operating room.
هل شُخِّصَ لديك انزلاقٌ غضروفي في مسقط؟ تُوصي الإرشادات الدولية بالعلاج التحفّظي أولاً. اكتشف العلاج غير الجراحي للديسك في مركز CBP للدقة في العمود الفقري.
تشخيصٌ لا يلزم بالضرورة أن ينتهي في غرفة العمليات
أجريتَ صورة الرنين المغناطيسي. جلستَ مقابل طبيب يُشير إلى بقعةٍ داكنة على الفحص ويقول الكلمات: انزلاقٌ غضروفي، أو ديسك، أو فتق القرص. ربّما أتبَعَ ذلك بتحويلةٍ إلى جرّاح عمودٍ فقري. ربّما ذكر استئصال القرص أو دمج الفقرات. ربّما عدتَ إلى المنزل مقتنعاً بأنّ الجراحة حتمية.
إن كنتَ تبحث عن إجاباتٍ في هذه اللحظة — تكتب "انزلاق غضروفي مسقط" أو "علاج الديسك بدون جراحة" أو "بدائل جراحة الديسك" في غوغل في وقتٍ متأخّر من الليل — فأنت لستَ وحدك. وقد لا تكون قد عُرِضَت عليك أهمّ حقيقةٍ بشأن تشخيصك.
وفقاً للإرشادات السريرية الدولية الصادرة عن لجنة العمود الفقري في الاتحاد العالمي لجمعيّات جراحة الأعصاب (WFNS)، فإنّ العلاج التحفّظي (غير الجراحي) هو العلاج الأوّل المُوصى به للانزلاق الغضروفي القطني في المرضى الذين لا يُعانون من علامات عجزٍ عصبيّ خطيرة محدّدة. وهذه التوصية صادرةٌ عن جرّاحي الأعصاب أنفسهم. هم ليسوا ضدّ الجراحة. هم يلتزمون بالأدلّة — والأدلّة واضحة.
الأدلّة لافتةٌ أيضاً بطريقةٍ أخرى: أكثر من 85% من المرضى الذين يُعانون من انزلاقٍ غضروفي حادّ مع ألمٍ عصبي تختفي أعراضهم مع الوقت بفضل الرعاية التحفّظية المناسبة. وفي أكثر من نصف الحالات، تمتصّ المادة الغضروفية المُنزلقة نفسها جزئياً أو كلّياً داخل الجسم — أي أنّ الانتفاخ المرئي على صورة الرنين المغناطيسي يمكن أن يتقلّص من تلقاء نفسه، إذا توفّرت الظروف المناسبة.
تُوضّح هذه المقالة ما هو الانزلاق الغضروفي فعلياً، وما الذي تُوصي به الإرشادات الدولية، ومتى تكون الجراحة ضرورية حقاً، وكيف يبدو العلاج التحفّظي في عيادتنا "مركز CBP للدقة في العمود الفقري" في مسقط.
ما الذي يعنيه "الانزلاق الغضروفي" فعلياً؟
مصطلح "الانزلاق الغضروفي" مفيدٌ ومُختصر، لكنّه مُضلّلٌ بعض الشيء. الأقراص الفقرية لا "تنزلق" خارج موضعها. فالأقراص بين كلّ زوجٍ من فقرات العمود الفقري مُثبَّتةٌ بإحكام. ما يحدث فعلياً أكثر تحديداً — وفهمه يُغيّر طريقة تفكيرك في العلاج.
كلّ قرصٍ يتكوّن من جزأين: حلقةٌ خارجيةٌ صلبة (الحلقة الليفية / Annulus Fibrosus) ولُبٌّ داخليٌّ هلامي (النواة اللبية / Nucleus Pulposus). حين تَضعُف الحلقة الخارجية أو تتمزّق، يستطيع اللبّ الداخلي الاندفاع للخارج عبر الجدار المُتضرّر. وبحسب مدى اندفاعه، يَصف الأطباء ذلك بأنّه:
- انتفاخ القرص — ضغطٌ خفيف على جدار القرص للخارج
- بروز القرص — تدفع المادة الداخلية على الجدار الخارجي دون أن تخترقه
- فتق القرص (الانزلاق الغضروفي) — تخترق المادة الداخلية الجدار الخارجي
- الاحتجاز أو الانفصال (Sequestration) — انفصال المادة وانتقالها بعيداً عن القرص
حين تضغط المادة المُنزاحة على جذر عصبٍ مجاور — وهو الأكثر شيوعاً في أسفل الظهر، فيُهيِّج العصب الوركي — تكون النتيجة ألماً يمتدّ إلى الساق، يُصاحبه عادةً وخز، أو خَدَر، أو ضعف. وهذا الجمع بين مشكلة القرص وتهيّج العصب هو ما يصفه كثيرون ببساطة بـ"ألم الانزلاق الغضروفي"، ويُعرف سريرياً بـالاعتلال الجذري القطني (Lumbar Radiculopathy)، أو بشكلٍ مألوفٍ أكثر، عرق النسا.
ما الذي تُوصي به الإرشادات الدولية فعلياً؟
هذا هو الجزء الذي لا يُخبَر به معظم المرضى في مسقط بشكلٍ مناسب.
تُعدّ لجنة العمود الفقري في الاتحاد العالمي لجمعيات جراحة الأعصاب (WFNS) من أكثر الهيئات الدولية موثوقيةً في الرعاية الصحية للعمود الفقري. وتوصيتها الرسمية بشأن الانزلاق الغضروفي القطني صريحة: "يُوصى بالعلاج التحفّظي بوصفه العلاجَ الأوّل للانزلاق الغضروفي القطني لدى المرضى الذين لا يُعانون من عجزٍ عصبيّ مثل العجز الحركي أو متلازمة ذيل الفرس."
وتُكرّر الإرشادات السريرية لجمعية العمود الفقري لأمريكا الشمالية (NASS) لعام 2022 الموقفَ ذاته: التدخّل الجراحي مُستطَبٌّ فقط للمرضى الذين يُعانون من ضعفٍ عصبيٍّ كبيرٍ أو مُتفاقم، أو ألمٍ مُستعصٍ لم يستجب للرعاية التحفّظية، أو تشوّهاتٍ بنيويةٍ محدّدة تستلزم تصحيحاً جراحياً.
فترة التجربة التحفّظية المعيارية قبل التفكير في الجراحة هي 4 إلى 6 أسابيع، وفي كثيرٍ من الإرشادات تصل إلى 8 أسابيع. وخلال هذه الفترة، تُظهر البيانات أنّ:
- أكثر من 85% من حالات الانزلاق الغضروفي الحادّ مع الألم العصبي تختفي أعراضها مع الوقت بفضل الرعاية غير الجراحية المناسبة
- يحدث الامتصاص التلقائي للمادة الغضروفية المُنزلقة في أكثر من نصف الحالات المصحوبة بأعراض التي يتمّ التعامل معها تحفّظياً — أي أنّ جسمك قادر، في الظروف المناسبة، على إعادة امتصاص المادة الغضروفية التي تُسبّب لك الألم حالياً
- الجراحة ليست الخيارَ الأوّل الافتراضي. إنّها خيارٌ مُخصَّصٌ للحالات التي خضعت لتجربةٍ تحفّظيةٍ عادلة وفشلت فيها، أو التي تظهر فيها علامات إنذار محدّدة منذ البداية
وما يعنيه ذلك عملياً: إن كنتَ قد شُخِّصتَ مؤخّراً بانزلاقٍ غضروفي ولا تُعاني من علامات الإنذار المحدّدة المذكورة أدناه، فإنّ الخطوة الأولى المناسبة سريرياً — وفقاً للإرشادات الدولية للجرّاحين أنفسهم — هي خوض دورةٍ مُنظَّمة من الرعاية التحفّظية. لا الجراحة الفورية.
متى تكون الجراحة ضرورية حقاً — علامات الإنذار التي لا يجوز تجاهلها
هذه المقالة ليست ضدّ الجراحة. الجراحة تُنقذ الناس. ثمّة حالاتٌ محدّدة يكون فيها التدخّل الجراحي ليس فقط مناسباً بل عاجلاً. إن انطبق عليك أيٌّ ممّا يلي، توقّف عن القراءة واطلب تقييماً طبياً طارئاً فوراً:
- أعراض متلازمة ذيل الفرس (Cauda Equina Syndrome): فقدان السيطرة على المثانة أو الأمعاء، أو خَدَرٌ في منطقة السرج/العانة، أو ضعفٌ شديد ومفاجئ في الساقين معاً
- عجزٌ عصبيٌّ تقدّمي: ضعفٌ متفاقم في الساق أو القدم (سقوط القدم، عدم القدرة على رفعها، ضمورٌ شديد في العضلات)
- ألمٌ شديد ومُستعصٍ لا يستجيب لأيّ إجراءٍ تحفّظي ويتفاقم بسرعة
- فقدانٌ مفاجئ للمنعكسات أو الإحساس بنمطٍ واضح يطابق جذرَ عصبٍ معيّن
هذه استطباباتٌ جراحيةٌ واضحة، وأيّ طبيبٍ مسؤول — ونحن منهم — سيُحوِّلك فوراً إلى جرّاح عمودٍ فقري إن كانت موجودة. وجرّاحو العظام والأعصاب في مستشفياتٍ مثل أبوللو، ومستشفى مسقط الخاص، والمستشفى السلطاني محترفون مَهَرَة، ونحن نعمل ضمن مساراتهم للتحويل حين تكون الجراحة مُستطَبَّةً فعلاً.
ما تتناوله هذه المقالة هو الفئة الأكبر بكثير من مرضى الانزلاق الغضروفي — ربّما 80 إلى 90 بالمئة من جميع الحالات — الذين لا يُعانون من علامات الإنذار هذه، والذين قيل لهم إنّهم "قد يحتاجون إلى جراحة"، ويستحقّون أن يعرفوا أنّ الإرشادات الدولية تنصّ على أنّ الرعاية التحفّظية يجب أن تأتي أولاً.
لماذا يَمتصّ كثيرٌ من مرضى الانزلاق الغضروفي حالاتهم دون جراحة؟
حقيقةُ أنّ القرص المُنزلق يستطيع التقلّص والامتصاص من تلقاء نفسه تُفاجئ معظم المرضى. وتُفاجئ بعض الأطبّاء أيضاً. لكنّها مُوثَّقة جيداً في الأدبيّات الطبية.
حين تندفع المادة الداخلية للقرص عبر الجدار الخارجي، يتعرّف الجسم على المادة المُنزاحة باعتبارها شيئاً لا ينتمي إلى خارج كبسولة القرص. تتحرّك الخلايا الالتهابية وتُفكّك تدريجياً المادةَ البارزة — وهي عملية امتصاصٍ طبيعية. وتُظهر الدراسات أنّ هذا يحدث في أكثر من نصف الحالات المصحوبة بأعراض التي تُدار تحفّظياً، بل إنّ بعض الأبحاث تُظهر معدّلات امتصاصٍ أعلى للانزلاقات الكبيرة مقارنةً بالصغيرة.
ولكي يحدث الامتصاص، يُساعد توفّر شرطين بشكلٍ كبير:
- تخفيف الضغط الميكانيكي على القرص المتأثّر — عبر المحاذاة السليمة للعمود الفقري، والتخفيف، وتجنّب الوضعيات التي تضغط الانزلاق أكثر
- تقليل الالتهاب الموضعي حول جذر العصب — يُدار بضبط الالتهاب، والعلاجات المُستهدَفة، واستعادة الحركة التدريجية
هذا بالضبط ما صُمِّم برنامج الرعاية التحفّظية المناسب لتقديمه. إنّه ليس انتظاراً سلبياً. بل خلقٌ نشطٌ للظروف التي يستطيع جسمك ضمنها أن ينجح في عمليات شفائه الطبيعية.
ما الذي ينبغي أن تشمله الرعاية التحفّظية فعلياً؟
ليست كلّ رعايةٍ تحفّظيةٍ متساوية. فالمريض الذي يُقال له "ارتح، خذ المُسكِّنات، وعد بعد شهر" لا يتلقّى علاجاً تحفّظياً قائماً على الأدلّة. بل يُقال له أن ينتظر — وهذا أمرٌ مختلف.
البرنامج التحفّظي المناسب للانزلاق الغضروفي، استناداً إلى الإرشادات الدولية والأدلّة السريرية، ينبغي أن يشمل:
1. تقييمٌ تشخيصيٌّ موضوعي. أخذ التاريخ المرضي المفصّل، والفحص السريري، والفحوص العصبية، ومراجعة التصوير. الهدف هو تحديد المستوى الفقري المتأثّر بدقّة، وأيّ جذرٍ عصبيّ متضرّر، وما إذا كانت ثمّة علامات إنذار تستلزم تحويلاً جراحياً فورياً.
2. إدارة الألم والالتهاب. قد تشمل، عند الحاجة، أدوية مضادّة للالتهاب لفترةٍ قصيرة، وبروتوكولات للثلج والحرارة، وأساليب علاجٍ مُستهدَفة. الهدف هو تقليل الالتهاب حول جذر العصب، لا إخفاء الألم بمسكّناتٍ بشكلٍ دائم.
3. التخفيف الميكانيكي (Mechanical Decompression). هذا أمرٌ بالغ الأهمية وكثيراً ما يكون مفقوداً من العلاج الطبيعي العام. الشدّ القطني والتخفيف المُطبّق بشكلٍ صحيح يستطيعان تقليل الضغط على القرص المتأثّر، وخلق الظروف الميكانيكية التي تدعم الامتصاص الطبيعي.
4. التصحيح الوضعي والبنيوي. نادراً ما يحدث الانزلاق الغضروفي على عمودٍ فقريّ متساوي المحاذاة. فالغالبية العظمى من مرضى القرص يحملون سنواتٍ من الخلل الوضعي المتراكم — انحناءات قطنية مُسطّحة، وميل أمامي للحوض، وضعف الجذع، أو تحوّلات تعويضية — وضعت حملاً غير متساوٍ على القرص حتى انهار. ودون تصحيح هذا الاختلال الكامن في المحاذاة، فحتى القرص المُمتَصّ كلّياً يكون عُرضةً عاليةً لإعادة الإصابة.
5. علاجٌ مُستهدَفٌ للأنسجة الرخوة والعضلات. حيث يكون التشنّج العضلي المزمن وتقييد اللفافة (Fascia) جزءاً من نمط الألم، يكون العلاج بالموجات التصادمية خارج الجسم قيِّماً. يُحفّز العلاج بالموجات التصادمية تدفّق الدم إلى مناطق الأنسجة الرخوة المزمنة ويُسرّع إصلاح الأنسجة — ممّا يجعله إضافةً مفيدة لكثيرٍ من حالات الانزلاق الغضروفي حيث أصبحت العضلات المحيطة مشدودةً أو مُلتهبةً مزمناً.
6. حركةٌ تقدّمية وإعادة تأهيل. تمارين مُسلسَلة بعنايةٍ لاستعادة استقرار العمود الفقري دون تفاقم القرص. وهنا تُخفق غالباً تمارين يوتيوب العامة في مساعدة المرضى — فما يُساعد نمطَ قرصٍ معيّن قد يُفاقم آخر، ويجب أن يكون التقدّم موجَّهاً.
7. تعديلٌ في نمط الحياة والأرغونوميا. كيف تجلس، وتنام، وتحمل الأشياء، وتتحرّك، يؤثّر في ما إذا كان قرصك يتعافى أم يزداد سوءاً. وأيّ خطّة رعايةٍ كاملةٍ تُعالج ذلك مباشرةً.
<u>منهج CBP</u>: لماذا يَهمّ التصحيح البنيوي لمرضى الانزلاق الغضروفي؟
هنا يُقدّم منهج Chiropractic BioPhysics® (CBP) ما لا تُقدّمه معظم برامج الرعاية التحفّظية في مسقط. وتُعدّ CBP أكثر تقنيات تقويم العمود الفقري التي خضعت للبحث في العالم، وتدعمها أكثر من 200 دراسة محكَّمة. ومبدؤها الأساسي هو التصحيح البنيوي الدقيق والقابل للقياس للعمود الفقري — وبالنسبة لمرضى الانزلاق الغضروفي، يَهمّ هذا كثيراً.
تحدث معظم حالات الانزلاق الغضروفي على عمودٍ فقريٍّ فقد بنيته الصحيحة على مدى سنوات. الانحناء القطني تسطّح. الحوض مال. الفقرات تجلس بزوايا لم تُصمَّم لها. وتحت ذلك الحِمل الميكانيكي غير الطبيعي، ينهار قرصٌ واحد في النهاية.
الرعاية التحفّظية العامة تستطيع تقليل الالتهاب وقد تسمح حتى بامتصاصٍ جزئي — لكن إن لم يُصحَّح النمط البنيوي الكامن الذي أدّى إلى انهيار القرص في المقام الأول، فمعدّلات تكرار الإصابة تكون عالية. يعود المرضى إلى المكتب نفسه، والوضعية نفسها، والاختلال نفسه، وفي غضون أشهرٍ أو سنوات، ينهار المستوى نفسه أو مستوى مجاور مرّةً أخرى.
يجمع علاج CBP للانزلاق الغضروفي بين:
- التصوير الرقمي بالأشعة السينية لقياس مدى انحراف العمود الفقري بالضبط عن المحاذاة المثالية
- تعديلات الصورة المرآوية (Mirror-Image Adjustments) المُطبَّقة في الاتجاه الدقيق المعاكس لنمط الاختلال الخاصّ بالمريض
- الشدّ القطني المُعايَر والتخفيف لتقليل الضغط على القرص المتأثّر وخلق ظروفٍ مواتيةٍ للامتصاص
- تمارينُ تصحيحيةٌ مُستهدَفة مُختارةٌ خصيصاً للنمط البنيوي للمريض، لا "تمارين ظهرٍ" عامة
- عند الحاجة، أساليبُ علاجٍ مُتكاملة بما في ذلك العلاج بالموجات التصادمية والعلاج بالليزر من الفئة الرابعة لضبط الالتهاب
الهدف مزدوج: حلّ نوبة القرص الحالية بوسائلَ تحفّظيةٍ حيثما أمكن، وتصحيح النمط البنيوي الكامن حتى لا ينهار القرص مرّةً أخرى.
كيف يبدو التعافي واقعياً؟
يستحقّ المرضى توقّعاتٍ صادقة. التعافي من الانزلاق الغضروفي ليس عمليةً تستغرق أسبوعاً، ونحن لا ندّعي ذلك. وفيما يلي المسار الواقعي لمعظم حالات القرص غير الجراحية في عيادتنا:
الأسبوعان 1–2: تقييمٌ شامل، ومراجعة للتصوير، وإدارة للأعراض الحادّة. الأولوية الأولى هي تقليل الالتهاب حول جذر العصب وتحديد أيّ علامات إنذار. ويبدأ معظم المرضى في الشعور ببعض الانخفاض في شدّة الألم خلال هذه الفترة، حتى قبل بدء التصحيح البنيوي.
الأسابيع 3–8: مرحلة العلاج النشط. جلستان إلى ثلاث جلسات أسبوعياً تجمع بين الشدّ والتخفيف، وتعديلات الصورة المرآوية، والأساليب المُستهدَفة، وبدء تمارين إعادة التأهيل. هذه هي الفترة التي يختبر فيها معظم المرضى زوالاً ملحوظاً للأعراض. وباتّباع إطار التجربة التحفّظية لـ 4–6 أسابيع المُوصى به دولياً، يتحسّن في نهاية هذه المرحلة الجزء الأكبر من المرضى الذين لا يُعانون من علامات إنذار تحسّناً جوهرياً.
الأشهر 3–6: مرحلة التثبيت والتصحيح البنيوي. تنخفض وتيرة العلاج. ويتحوّل التركيز إلى تصحيح النمط الوضعي والبنيوي الكامن الذي سمح بانهيار القرص. وتُؤكّد إعادة التصوير، حيث يكون مناسباً، التغيّرَ البنيوي.
المتابعة المستمرّة: مراجعاتٌ دورية للحفاظ على التصحيح طويل المدى ومنع التكرار في المستوى نفسه أو المستويات المجاورة.
إذا لم يتقدّم المريض في أيّ مرحلةٍ من هذا الجدول الزمني كما هو متوقّع، أو إذا ظهرت علامات إنذار، فإنّنا نُحيله للاستشارة الجراحية. هذا ليس فشلاً للرعاية التحفّظية — بل تطبيقٌ مسؤولٌ للإرشادات السريرية، التي تُقرّ هي نفسها بأنّ بعض المرضى يحتاجون إلى الجراحة.
متى ينبغي عليك حجز استشارة؟
ينبغي عليك التفكير في تقييمٍ للرعاية التحفّظية في عيادتنا إذا:
- شُخِّصتَ مؤخّراً بفتق قرص، أو انزلاقٍ غضروفي، أو تدلّي قرص، وتستكشف الخيارات قبل الجراحة
- كنتَ ضمن نافذة 4–8 أسابيع منذ بداية الأعراض ولم تخضع بعد لتجربةٍ تحفّظيةٍ مُنظَّمة
- تُعاني من ألم في الساق، أو خَدَر، أو وخز إلى جانب آلام أسفل الظهر (الاعتلال الجذري القطني / عرق النسا)
- قيل لك إنّك "قد تحتاج إلى جراحة" لكنّك تريد أن تفهم ما إذا كانت الرعاية التحفّظية مناسبة أولاً
- خضعتَ بالفعل لجراحةٍ سابقة على العمود الفقري وتريد منع إعادة الإصابة في مستويات الأقراص المجاورة
- تريد تقييماً قابلاً للقياس ويستند إلى التصوير لعمودك الفقري، لا مجرّد إدارة الأعراض
ينبغي عليك عدم تأجيل التقييم الجراحي إذا كانت أيٌّ من علامات الإنذار المذكورة سابقاً موجودة. سنُحيلك فوراً إن كانت كذلك.
كلمةٌ أخيرة بشأن قرار الجراحة
قرار إجراء جراحةٍ على العمود الفقري من أهمّ القرارات الطبية التي يمكن أن يتّخذها الإنسان. ويستحقّ أن يُتَّخَذ بمعلوماتٍ كاملة.
الجراحة هي الخيار الصحيح لبعض مرضى الانزلاق الغضروفي — خاصةً أولئك الذين تظهر لديهم علامات إنذار، أو لديهم تقدّمٌ عصبيٌّ مُؤكَّد، أو الحالات التي فشلت فيها تجربةٌ تحفّظيةٌ كافية. بالنسبة لهؤلاء المرضى، فإنّ جراحة العمود الفقري الحديثة في عُمان ممتازة، ويمكن أن تكون مُنقذةً للحياة.
لكنّ الإرشادات الدولية لا لبس فيها: الجراحة ليست الخطوة الأولى الصحيحة لمعظم مرضى الانزلاق الغضروفي. الرعاية التحفّظية هي. وإن كنتَ تقرأ هذه المقالة لأنّه قيل لك إنّك قد تحتاج إلى جراحة، فأنت تَدين لنفسك — على الأقلّ — بأن تفهم ما الذي يستطيع برنامج رعايةٍ تحفّظيةٍ مُنظَّمٍ بشكلٍ صحيح أن يُنجزه لك أوّلاً.
نحن <u>أول عيادة معتمدة في تقنية Chiropractic BioPhysics® (CBP) في المنطقة</u>، ونُعالج حالات الانزلاق الغضروفي بانتظام باستخدام مبادئ الرعاية التحفّظية المُعترَف بها دولياً. ونعمل ضمن المسارات الجراحية حين تكون الجراحة مُستطَبَّةً فعلاً، ولا ندّعي أنّ الرعاية التحفّظية مناسبة لكلّ حالة. ولكنّنا نُؤمن بأنّ كلّ مريض قرصٍ يستحقّ فرصة تجربة الرعاية التحفّظية أوّلاً، بالطريقة التي تُوصي بها الإرشادات الدولية.
احجز استشارتك للانزلاق الغضروفي اليوم — واكتشف ما إذا كانت حالتك من تلك التي يمكن أن تُحلّ دون دخول غرفة العمليات أبداً.
سلطنة عمان - مسقط - العذيبة
شارع 18 نوفمبر - فيلا 336